Spondylosis Symptoms and Treatment: Causes and Evidence-Based Options
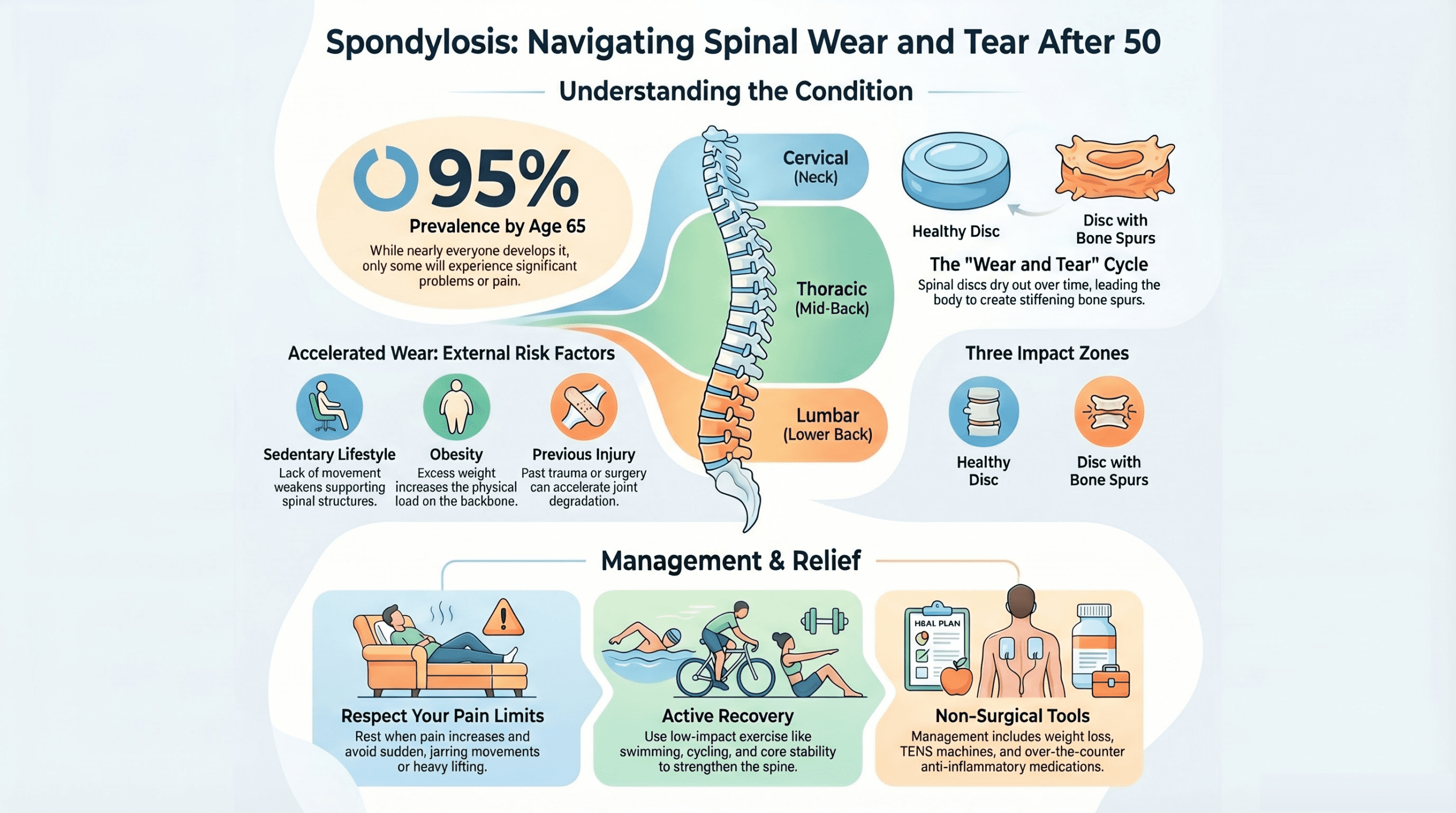
Understanding spondylosis symptoms and treatment options is essential for the over 50s across the UK, as spondylosis is one of the most common causes of spine pain and stiffness. Everyday wear and tear damages your spinal joints, and you are increasingly likely to develop the condition as you age. Research suggests that 95% of people will develop some degree of spondylosis by the age of 65-yet most experience only mild or no symptoms at all.
Understanding what spondylosis is, how it develops, and what treatment options are available (both NHS and private) can help you manage the condition effectively and stay active.
What is Spondylosis?
Spondylosis, also called spinal osteoarthritis, is degeneration of the spine caused by age-related wear and tear. Your spine is a column of bones called vertebrae, separated and cushioned by discs. Over time, these discs dry out, lose their flexibility, and become prone to damage. Your body responds by forming small bone spurs (osteophytes) to stabilise the affected joints.
This combination-disc loss and bone spur formation-makes the spine stiffer and less flexible. The severity varies greatly from person to person. Some people experience no symptoms at all, whilst others have persistent, disabling pain.
Types of Spondylosis by Location
Spondylosis is classified by which region of the spine is affected:
- Cervical spondylosis: Affects the neck. Can cause neck pain, stiffness, and pain or numbness radiating into the shoulders, arms, and hands.
- Thoracic spondylosis: Affects the mid-back (less common and usually causes mild symptoms).
- Lumbar spondylosis: Affects the lower back. Often causes lower back pain, stiffness, and sometimes pain or weakness in the legs and buttocks.
Watch: Spondylosis Causes, Symptoms and Treatment Guide
Watch our cinematic overview covering the key causes of spondylosis, how symptoms develop, and the evidence-based treatment options available on the NHS and privately in the UK – helping you make informed decisions about your spinal health after 50.
What Causes Spondylosis?
Spondylosis develops through a natural process of ageing, but several factors accelerate or worsen the condition.

Primary Cause: Age-Related Disc Degeneration
As you age, the discs between vertebrae gradually lose water content and become less resilient. The collagen fibres that support them weaken, making the discs more susceptible to cracks and tears. This process is inevitable and begins in most people by their 30s or 40s, though symptoms typically appear later.
Secondary Risk Factors
Several lifestyle and health factors increase your risk of developing symptomatic spondylosis:
- Obesity or being overweight (increased load on the spine)
- Sedentary lifestyle (weak supporting muscles)
- Previous spinal injury or surgery
- Repeatedly carrying heavy weights or poor lifting technique
- Existing severe arthritis elsewhere in the body
- Psychological stress, anxiety, or depression (linked to muscle tension and pain perception)
- Smoking (reduces blood flow to discs)
Spondylosis Symptoms and Treatment: What to Look For
Most people with spondylosis have no symptoms. However, when symptoms do occur, they can include:
- Spinal joint pain or tenderness that comes and goes
- Stiffness, especially in the morning or after periods of inactivity
- Muscle spasm and pain around the affected area
- Loss of balance or difficulty walking (if lumbar spondylosis affects leg nerves)
- A grinding or popping sensation in the spine when moving
- Headaches (in cervical spondylosis)
- Numbness, tingling, or weakness in the arms or legs (if nerve compression occurs)
Symptoms vary widely. Some people experience only mild, intermittent discomfort, whilst others have continuous pain that limits daily activities. If you develop numbness, tingling, or weakness (especially sudden onset), contact your GP urgently, as this may indicate nerve compression.
NHS vs Private Diagnosis and Treatment
NHS Pathway
On the NHS, spondylosis diagnosis typically begins with your GP, who will take a history and perform a physical examination. They may order X-rays (usually free) to confirm the diagnosis. If nerve compression is suspected, an MRI scan may be arranged (waiting time typically 6-12 weeks depending on your area). If your GP also wants to check for osteoporosis, which can coexist with spondylosis, you may be referred for a DEXA bone density scan.
Treatment on the NHS focuses on managing symptoms:
| Treatment | Cost (NHS) | Availability |
|---|---|---|
| Paracetamol or ibuprofen | Free | Immediate |
| Stronger painkillers (codeine, tramadol) | Free (prescription charge £9.90) | Via GP |
| Muscle relaxants | Free (prescription charge) | Via GP |
| Steroid injection (into facet joints) | Free | 6-8 weeks (via specialist) |
| Physiotherapy (typically 6-8 sessions) | Free | 2-4 weeks (via GP referral) |
| Surgery (if nerve compression) | Free | 3-6 months waiting list |
Private Pathway
Private treatment offers faster access to imaging and specialists:
- Private GP consultation: £100-£150
- Private MRI scan: £300-£500 (next-day or same-day availability)
- Specialist spinal physician consultation: £200-£300
- Private steroid injection: £400-£600
- Private physiotherapy: £40-£60 per session
- Surgery (decompression, fusion, or disc replacement): £8,000-£15,000+ depending on complexity
Many people choose private treatment for faster diagnosis and steroid injections, then return to NHS care for ongoing management.
Evidence-Based Management Strategies
Most cases of spondylosis do not require surgery. Understanding spondylosis symptoms and treatment approaches helps you manage the condition effectively through self-care. Here are proven approaches:
Pain Management
Over-the-counter paracetamol (up to 1,000 mg four times daily) or ibuprofen (up to 400 mg three times daily) can provide relief. Non-steroidal anti-inflammatory drugs (NSAIDs) are particularly helpful during flare-ups. If you have stomach issues or take other medications, consult your pharmacist before using NSAIDs regularly.
Keep Moving: Exercise and Activity
Contrary to old advice to rest, staying active is crucial. Regular gentle movement keeps your spine mobile, strengthens supporting muscles, and reduces pain. Recommended activities include:
- Walking (30 minutes daily)
- Swimming or water aerobics (excellent for unloading the spine)
- Cycling (low-impact and spine-friendly)
- Core stability exercises (Pilates, yoga)
Start gently and build gradually. A physiotherapist can provide bespoke exercises tailored to your affected spinal region.
Weight Management
If you are overweight, losing weight reduces the load on your spine. Even a 5-10% reduction in body weight can significantly improve pain and function.
Posture and Ergonomics
Poor posture accelerates spondylosis and worsens symptoms. When sitting, keep your shoulders relaxed, your back supported, and your screen at eye level. Avoid prolonged static positions-move every 30-45 minutes.
Heat and Cold Therapy
Heat (via a hot water bottle or heat pad) relaxes muscles and improves flexibility. Cold therapy reduces acute inflammation during flare-ups. Alternate between them as needed.
TENS Machines
Transcutaneous electrical nerve stimulation (TENS) devices can provide pain relief in the comfort of your own home. Portable TENS units cost £20-£50 and are available over the counter. They work by blocking pain signals to the brain.
Sleep Optimisation
Good sleep reduces pain perception and supports healing. Use a supportive pillow that aligns your neck, sleep on your back or side (not prone), and maintain a cool bedroom.
When to Seek Professional Help
Contact your GP if you develop any of the following symptoms. Your GP can use the NHS e-Referral Service to refer you to a spinal specialist if needed:
- New or worsening numbness or tingling in your arms or legs
- Weakness in your limbs
- Loss of bladder or bowel control (seek urgent care)
- Fever or unexplained weight loss (suggests a different condition)
- Pain that does not improve with over-the-counter medication after 4 weeks
Frequently Asked Questions
Is spondylosis curable?
No-spondylosis is a permanent age-related change. However, symptoms can be effectively managed through exercise, lifestyle changes, and medication. Many people experience long periods of remission.
Can spondylosis get worse?
Yes, it can progress, but progression is usually slow. Staying active, maintaining a healthy weight, and avoiding heavy lifting or smoking can slow deterioration.
Is surgery necessary?
Surgery is rarely needed. It is only considered when nerve compression causes persistent numbness, weakness, or loss of function despite conservative treatment. Our guide to the most common surgeries for over-50s covers NHS costs and private options if surgery does become necessary. Most people manage well without surgery.
How long will I have pain?
This varies widely. Some people have occasional pain for years, whilst others experience flare-ups. Most people find that symptoms improve with regular exercise and activity.
Can I return to normal activities?
Yes, with proper management. Avoid heavy lifting and high-impact activities (like running), but walking, swimming, cycling, and most daily activities are fine.
Are steroid injections safe?
Yes, when given by trained professionals. Injections provide temporary relief (typically 2-3 months) and allow you to engage in physiotherapy and exercise more comfortably. Repeated injections are limited to 3-4 per year to minimise systemic steroid exposure.
Key Takeaways
- Spondylosis is age-related spinal degeneration affecting 95% of people by age 65, but most experience no symptoms.
- Symptoms (pain, stiffness, rarely nerve compression) vary widely and can be effectively managed through lifestyle changes and medication.
- NHS treatment is free and includes physiotherapy, medication, and injections; private care offers faster access to imaging and specialists.
- Exercise, weight management, good posture, and activity are the most effective long-term management strategies.
- Surgery is rarely needed and only considered for nerve compression with persistent weakness or loss of function.
- Most people with spondylosis can remain active, work, and enjoy a normal quality of life with proper management.
Further Support and Resources
For evidence-based information about managing spondylosis and arthritis, visit the Versus Arthritis website, which offers comprehensive guides on both conditions. The NHS also provides detailed information on cervical spondylosis and osteoarthritis.
If your symptoms worsen or you develop new neurological symptoms, contact your GP promptly. Early assessment can prevent complications and identify the most appropriate treatment pathway-whether NHS or private.
This article is for information only. Always consult your GP or a qualified healthcare professional before making health decisions.