Lupus Symptoms in Adults Over 50: What You Need to Know
If you’re over 50 and experiencing persistent joint pain, unexplained fatigue, or unusual skin rashes, lupus may be on your mind-or your GP’s. Lupus (systemic lupus erythematosus, or SLE) is a chronic autoimmune disease that can develop or flare for the first time in older adulthood.
Yet late-onset lupus is often missed or misdiagnosed because symptoms overlap with other age-related conditions like arthritis and thyroid disease.
This guide explains lupus symptoms, how diagnosis works on the NHS, private diagnostic options, and what you can do right now to get answers and take control of your health.
Around 50,000 people in the UK live with lupus, and though it affects women nine times more often than men, anyone can develop it-at any age.
What Is Lupus? Understanding Systemic Autoimmune Disease
Lupus is a chronic condition in which your immune system becomes overactive and attacks your body’s own healthy tissue. This self-directed immune response triggers inflammation, swelling, and tissue damage across multiple organs-including your joints, skin, kidneys, heart, and lungs.
Unlike other autoimmune diseases (such as rheumatoid arthritis, which mostly affects joints), lupus can strike almost anywhere in the body. This is why lupus symptoms are so varied and why diagnosis can take time. Your GP may initially suspect other conditions because lupus mimics symptoms of fibromyalgia, chronic fatigue syndrome, and other long-term illnesses.
The exact cause of lupus remains unclear, but research points to a combination of genetic, hormonal, and environmental triggers. Family history, viral infections, prolonged sun exposure, and hormonal changes (including pregnancy and the menopause) can all play a role. This is especially important for over-50s: late-onset lupus is becoming more recognised, and hormonal shifts in older age may contribute.
Watch: Lupus Symptoms After 50 – NHS vs Private Diagnosis and Treatment
This cinematic overview covers the key signs of lupus in older adults, how late-onset lupus is often misdiagnosed, NHS and private rheumatology pathways, treatment options, and practical advice for living well with lupus after 50.
The Main Types of Lupus Explained
Not all lupus is the same. There are three main types:
Systemic Lupus Erythematosus (SLE)
SLE is the most common type and what most people mean when they say “lupus.” It can affect any organ or tissue in your body. SLE significantly impacts quality of life through pain, fatigue, anxiety, and depression. Most people diagnosed with lupus have SLE.
Discoid Lupus Erythematosus (DLE)
DLE is a milder form that typically affects only the skin. Symptoms include red, circular, scaly patches (often on the face, scalp, or ears), hair loss, and bald patches. DLE rarely progresses to systemic disease, but sufferers must avoid direct sunlight to prevent flare-ups.
Drug-Induced Lupus
More than 100 medications can cause lupus-like symptoms, including some heart medications, antibiotics, and immunosuppressants. The good news: drug-induced lupus usually resolves once the offending medication is stopped or switched under medical guidance.
You may also find our guide to spondylosis symptoms and treatment: causes and evidence-based options helpful.
You may also find our guide to warning signs of a stroke to look out for helpful.
You may also find our guide to effective tips for preventing back pain helpful.
You may also find our guide to advice for living with fibromyalgia helpful.
You may also find our guide to thyroid problems could be the cause of your fatigue & weight gain helpful.
You may also find our guide to chronic pain and exercise: a few tips to improve your quality of life helpful.
You may also find our guide to noise-induced hearing loss – a comprehensive guide helpful.
You may also find our guide to how effective is exercise in managing fibromyalgia? helpful.
You may also find our guide to new research into the diagnosis and treatment of fibromyalgia helpful.
You may also find our guide to what makes a healthy diet? helpful.
You may also find our guide to 8 reasons to add swimming to your routine helpful.
You may also find our guide to oversleeping: causes and side effects helpful.
You may also find our guide to boost your brain and get smart: the cognitive benefits of stopping … helpful.
Common Lupus Symptoms: A Practical Overview
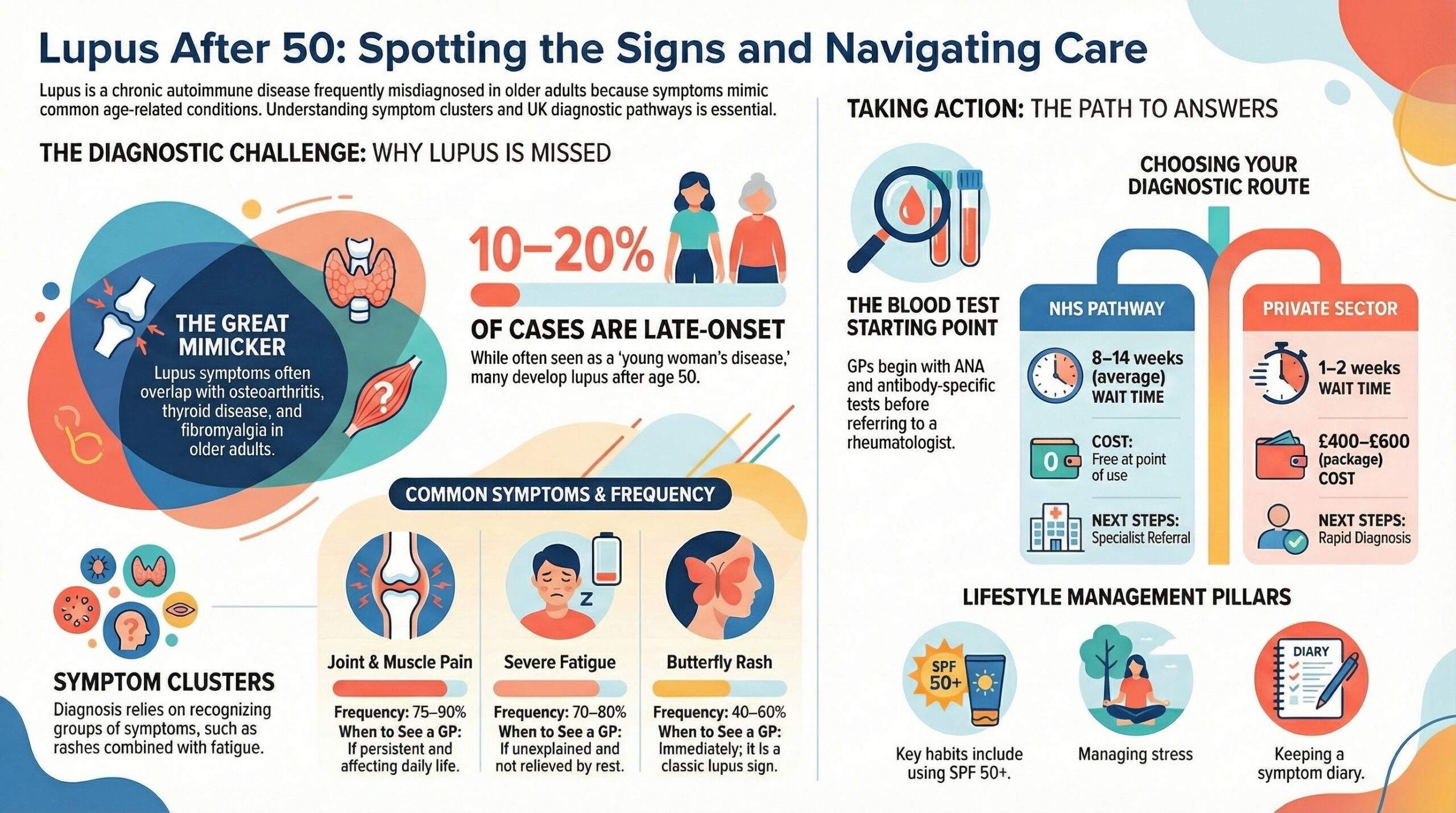
Lupus symptoms vary widely from person to person. Some people experience a few mild symptoms; others develop severe, multi-organ involvement. The key is recognising the pattern: lupus often causes clusters of symptoms rather than a single complaint.

Below is a table of the most common lupus symptoms, how often they occur, and when you should contact your GP:
| Symptom | Frequency in SLE Patients | When to See Your GP |
|---|---|---|
| Joint and muscle pain (arthralgia) | 75-90% | If persistent and affecting daily activities |
| Fatigue (often severe and debilitating) | 70-80% | If unexplained and not relieved by rest |
| Butterfly-shaped rash (malar rash) across cheeks and nose | 40-60% | Immediately; classic lupus sign |
| Swollen joints (arthritis) | 50-70% | If painful and affecting multiple joints |
| Unexplained fever (above 38C / 100.4F) | 30-50% | If recurring without infection or obvious cause |
| Hair loss (alopecia) | 25-40% | If sudden or in patches; may indicate flare |
| Mouth or nose ulcers (oral ulcers) | 20-35% | If recurring or painful; often painless in SLE |
| Raynaud’s phenomenon (pale/painful fingers in cold) | 15-30% | If new or severe; suggests autoimmune disease |
| Shortness of breath (dyspnoea) | 20-40% | Immediately; may indicate lung or heart involvement |
| Anaemia (low red blood cell count) | 25-35% | If causing breathlessness, dizziness, or pallor |
| Swollen lymph glands (lymphadenopathy) | 20-30% | If painless and persistent |
| Depression and anxiety | 30-40% | If new onset or worsening; may be disease or medication-related |
| Memory loss or cognitive fog (“lupus fog”) | 20-30% | If affecting work or daily tasks |
| Headaches or migraines | 25-35% | If new pattern, severe, or associated with neurological symptoms |
Important note: Lupus is not contagious. Many people experience only a few of these symptoms, whilst others develop new ones over time. Symptoms tend to flare (worsen suddenly) and then enter remission (improve). This unpredictable cycle is one reason lupus can be psychologically taxing alongside its physical effects.
Lupus Diagnosis: What to Expect in the NHS and Private Sector
Getting a lupus diagnosis takes time. Because symptoms overlap with other conditions and lupus is rarer in older patients, your GP may explore other diagnoses first. However, the diagnostic pathway is well established.
The NHS Diagnostic Pathway
If your GP suspects lupus, they will:
- Take a full history: Symptoms, family history, medication, and lifestyle factors.
- Order initial blood tests: Full blood count (FBC), urea and electrolytes (U&E), liver function tests (LFTs), and inflammatory markers (ESR, CRP).
- Request antinuclear antibody (ANA) testing: A positive ANA is highly suggestive of lupus but not diagnostic on its own. Around 95% of SLE patients have a positive ANA test.
- Arrange antibody-specific tests: Anti-double-stranded DNA (anti-dsDNA) and anti-Smith (anti-Sm) antibodies are specific to lupus. Finding these confirms the diagnosis.
- Refer to rheumatology: Once blood tests suggest lupus, your GP will refer you to an NHS rheumatologist for specialist assessment and confirmation.
NHS waiting times for rheumatology referral: As of 2026, the average wait for a rheumatology appointment following a GP referral is 8-14 weeks. In some areas, waits exceed 20 weeks. Once with the rheumatologist, you may wait another 2-4 weeks for blood test results and confirmation of diagnosis.
Private Sector Diagnosis
If you prefer faster diagnosis and assessment, you can see a private rheumatologist without an NHS referral. Private consultants can order the same blood tests and provide specialist evaluation more quickly.
Typical private rheumatology costs (2026):
- Initial private rheumatology consultation: £200-£350
- Follow-up consultation: £150-£250
- Blood tests (ANA, anti-dsDNA, etc.): £150-£300
- Combined package (consultation + bloods): £400-£600
Many private rheumatologists work within NHS trusts as well, so you may be able to have some tests done on the NHS whilst seeing a private consultant for faster assessment. Once diagnosed privately, you can return to NHS care for ongoing treatment and monitoring.
NHS vs Private: Comparison Table
| Factor | NHS | Private |
|---|---|---|
| GP to rheumatology referral | 8-14 weeks average; up to 20+ weeks in some areas | 1-2 weeks; often within days |
| Initial consultation cost | Free (after GP visit) | £200-£350 |
| Blood tests | Free on NHS | £150-£300 (may be separate) |
| Total diagnostic cost | £0 (except GP appointment) | £400-£600 for first diagnosis |
| Ongoing treatment | Free prescriptions (on exemption) | Private costs; can use NHS for follow-up |
| Specialist choice | Limited by local NHS trusts | Wide choice of consultants |
Late-Onset Lupus: Why Over-50s Are Often Misdiagnosed
Lupus has a reputation as a young woman’s disease. Most diagnoses occur between ages 15 and 45. However, late-onset lupus-developing after age 50-is increasingly recognised, and when it does appear in older adults, doctors often miss it.
Why Late-Onset Lupus Is Overlooked
Several factors mean over-50s are at risk of delayed or missed diagnosis:
- Symptom overlap: Fatigue, joint pain, and swollen joints are common in older age generally. These mimic osteoarthritis, rheumatoid arthritis, and thyroid disease.
- Subtle presentation: Late-onset SLE often has fewer positive antibodies and different organ involvement than early-onset lupus. Blood tests may be borderline positive.
- Multi-morbidity: Older adults often have several conditions at once (high blood pressure, diabetes, etc.), making it hard to isolate lupus as the main culprit.
- Medical bias: Some clinicians assume lupus doesn’t occur in older age, so they don’t test for it.
If you’re over 50 and have experienced a sudden worsening of joint pain, new rashes, or unexplained fatigue-especially alongside a family history of autoimmune disease-ask your GP specifically about lupus. Mention any new or unusual symptoms, and request ANA testing if it hasn’t been done.
Lupus Flares: Recognising When Your Condition Is Worsening
A lupus flare is a sudden worsening of symptoms after a period of relative calm. Flares can last days, weeks, or longer.
Common Flare Triggers
- Sun exposure or UV light (including fluorescent office lighting)
- Stress, emotional upheaval, or major life changes
- Infection (flu, urinary tract infection, dental procedures)
- Hormonal changes (menstruation, menopause transition, hormone replacement therapy)
- Certain medications (some antibiotics, NSAIDs)
- Stopping or reducing lupus medications prematurely
- Overexertion or inadequate rest
Warning Signs of a Flare
Watch for increased pain, new rashes, severe fatigue, fever, swollen glands, or unusual symptoms. If you suspect a flare, contact your rheumatology team promptly. Early intervention can prevent complications.
How Lupus Is Treated: Options on the NHS and Beyond
Although there is no cure for lupus, modern treatments are highly effective at controlling symptoms, preventing flares, and protecting organs from long-term damage. The goal of treatment is to allow you to lead an active, fulfilling life with minimal medication side effects.
Your rheumatologist will personalise your treatment based on your age, overall health, symptom severity, and organ involvement. Our guide to private scan costs in the UK covers what you might pay if you choose to fast-track diagnostic tests privately.
Medications for Lupus
Hydroxychloroquine (Plaquenil) is the cornerstone of lupus treatment. This medication slows disease progression, manages skin and joint symptoms, and protects against organ damage. Many people tolerate hydroxychloroquine well, and it does not cause the weight gain sometimes seen with corticosteroids.
Non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen reduce joint pain and inflammation. NSAIDs are usually used short-term during flares or for specific pain relief. Long-term NSAID use can increase cardiovascular and kidney risk, so they’re monitored carefully.
Corticosteroids (e.g. prednisolone) reduce inflammation and provide rapid symptom relief during flares. Steroids are often started at higher doses and then tapered to the lowest effective dose, because long-term high-dose steroids increase the risk of infections, bone loss, and weight gain.
Immunosuppressants such as azathioprine or mycophenolate mofetil suppress the overactive immune system, especially when lupus affects the kidneys or other vital organs.
Biologic therapies including rituximab and belimumab target specific parts of the immune system. They are increasingly used for more severe lupus or when other treatments haven’t worked. The UK is currently trialling new combinations of these drugs (e.g. rituximab + belimumab) in the 2026 STRATIFY Lupus trial, with early results suggesting significantly improved outcomes for patients with specific antibody profiles.
Managing Lupus Beyond Medication
Lifestyle measures are just as important as medication for controlling lupus:
- Sun protection: Wear broad-spectrum SPF 50+ sunscreen, a hat, and UV-blocking sunglasses daily. Avoid prolonged sun exposure and reduce exposure to fluorescent lighting where possible.
- Low-impact exercise: Walking, cycling, swimming, and yoga help maintain muscle strength, prevent bone loss, and boost mood. Aim for 30 minutes of gentle activity most days.
- Stress management: Stress triggers flares in many people. Try mindfulness, meditation, or counselling. The NHS offers free cognitive behavioural therapy (CBT) for long-term conditions via talking therapies services.
- Healthy diet: A balanced diet rich in vegetables, fish, whole grains, and lean protein supports overall health and may reduce inflammation. Some people find a Mediterranean diet helpful.
- Adequate rest: Pace yourself by alternating activity and rest. Most lupus patients benefit from 8-10 hours of sleep and afternoon rest periods.
- Avoid smoking and excess alcohol: Smoking impairs circulation and worsens lupus symptoms. Alcohol can interact with medications and increase infection risk.
- Keep a symptom diary: Tracking symptoms helps identify flare triggers and shows patterns to your rheumatologist.
Complications: When Lupus Affects Other Organs
One of the reasons lupus requires specialist care is the risk of organ involvement:
- Kidney disease (lupus nephritis): About 30-50% of people with SLE develop kidney involvement. Early detection through urine and blood tests is crucial; untreated lupus nephritis can lead to kidney failure.
- Heart disease: Lupus increases the risk of heart inflammation (myocarditis) and premature coronary artery disease. People with lupus should have regular heart monitoring.
- Lung disease: Shortness of breath can indicate lung inflammation. Pleurisy (inflammation of the lung lining) and interstitial lung disease occur in a minority of patients.
- Blood clots: Lupus increases the risk of deep vein thrombosis (DVT) and pulmonary embolism (PE). Anticoagulation may be needed.
- Neurological involvement: Lupus can affect the brain and central nervous system, causing cognitive problems, headaches, or (rarely) seizures.
Routine monitoring with blood tests and kidney function checks helps catch these complications early. Our guide to warning signs of illness and when to see your doctor covers the key symptoms you should never ignore.
Questions to Ask Your GP
If you suspect lupus, take a list of questions to your GP appointment. This ensures you get the information you need and makes the best use of your time:
- Could my symptoms be caused by lupus? What other conditions might present similarly?
- Will you test for antinuclear antibodies (ANA) and specific antibodies (anti-dsDNA, anti-Sm)?
- If my tests are positive, how soon can I be referred to a rheumatologist?
- Are there any medications I’m taking that could cause lupus-like symptoms (drug-induced lupus)?
- What should I monitor at home, and when should I contact you or the rheumatology team?
- Are there lifestyle changes I can make now whilst waiting for specialist assessment?
- Will I need regular blood tests and monitoring once diagnosed?
- How will treatment affect my other medications or health conditions?
- What support services are available (e.g. counselling, patient groups, rheumatology nurse helplines)?
- Can you refer me to Lupus UK or a local patient support group?
Frequently Asked Questions
What are the first signs of lupus in older adults?
The most common early signs include persistent fatigue that does not improve with rest, joint pain and stiffness (especially in the hands, wrists, and knees), unexplained skin rashes, and sensitivity to sunlight. In adults over 50, these symptoms are often mistaken for osteoarthritis, fibromyalgia, or normal ageing, which can delay diagnosis.
Can you develop lupus after the age of 50?
Yes. Late-onset lupus, diagnosed after age 50, accounts for roughly 10 to 20 per cent of all lupus cases. It tends to present differently from younger-onset lupus, with less kidney involvement but more lung and blood-related symptoms. If you have unexplained fatigue, joint pain, or recurring rashes, ask your GP about lupus testing.
How is lupus diagnosed in the UK?
Diagnosis usually starts with blood tests ordered by your GP, including an antinuclear antibody (ANA) test and a full blood count. If results suggest lupus, you will be referred to a rheumatologist for further testing, which may include anti-dsDNA antibodies, complement levels, and urine tests. On the NHS, the referral typically takes 6 to 18 weeks depending on your area.
Is there a cure for lupus?
There is currently no cure for lupus. Treatment focuses on controlling symptoms, preventing flares, and protecting organs from damage. Most people with lupus manage their condition with a combination of medications, lifestyle adjustments, and regular monitoring by a rheumatologist. Many people with lupus lead full, active lives with proper management.
What is the difference between lupus and fibromyalgia?
Both conditions cause fatigue and widespread pain, which is why they are often confused. Lupus is an autoimmune disease where the immune system attacks healthy tissue, causing inflammation and potential organ damage. Fibromyalgia is a chronic pain condition without inflammation or organ involvement. Blood tests for autoimmune markers (ANA, anti-dsDNA) help distinguish the two. It is possible to have both conditions at the same time.
Can I get private treatment for lupus in the UK?
Yes. You can see a private rheumatologist for faster diagnosis and ongoing management. An initial private consultation typically costs £200 to £350, with follow-up appointments around £150 to £250. Private blood tests for lupus panels cost £100 to £300. Many patients use private care for the initial diagnosis and faster specialist access, then transfer back to NHS care for long-term monitoring and medication.
Key Takeaways
- Lupus is a chronic autoimmune disease that can affect any part of your body. Symptoms vary widely and are often misdiagnosed as other conditions in older adults.
- Late-onset lupus (after age 50) is increasingly recognised but frequently overlooked. If you have unexplained fatigue, joint pain, and rashes, ask your GP about lupus testing.
- Diagnosis involves blood tests: ANA testing is the first step; positive anti-dsDNA and anti-Sm antibodies confirm the diagnosis. Specialist rheumatology assessment is essential.
- NHS rheumatology waiting times are 8-14 weeks on average; private diagnosis costs £400-£600 but is faster (1-2 weeks). Both pathways are valid.
- Modern treatments are highly effective. Hydroxychloroquine is the foundation; NSAIDs, steroids, and biologic therapies are tailored to your needs. Most people achieve good disease control.
- Lifestyle measures are crucial: Sun protection, low-impact exercise, stress management, and adequate rest support medication and improve quality of life.
- Lupus complications (kidney disease, heart disease, blood clots) require regular monitoring. Early detection and treatment prevent serious organ damage.
- With proper care and treatment, most people with lupus have a normal lifespan and can lead active, fulfilling lives. The key is early diagnosis, specialist care, and partnership with your healthcare team.
Living Well With Lupus: Your Action Plan
If you’ve been newly diagnosed with lupus-or suspect you might have it-here’s what to do now:
- Book a GP appointment: Bring a list of your symptoms and ask for ANA testing if it hasn’t been done. Request a rheumatology referral.
- Gather your medical history: Note when symptoms started, any family history of autoimmune disease, and current medications.
- Keep a symptom diary: Record daily fatigue levels, pain, rashes, and any potential triggers (sun exposure, stress, illness).
- Consider sun protection now: Buy high-SPF sunscreen and UV-blocking sunglasses-these help prevent flares whether or not you have lupus.
- Connect with others: Join Lupus UK or an online support community. Hearing from others with lived experience is invaluable.
- Prepare questions for your rheumatologist: Use the list above. Write down your biggest concerns and priorities for treatment.
- Explore support services: Ask your GP about access to physiotherapy, occupational health, counselling, and rheumatology nurse helplines.
Useful Resources and Sources
The following organisations and websites provide reliable, evidence-based information about lupus in the UK:
- Lupus UK – Charity dedicated to lupus support, information, and advocacy. Offers patient guides, local support groups, and a helpline.
- NHS.uk – Lupus Overview – Official NHS information on symptoms, diagnosis, and treatment in the UK health system.
- NICE (National Institute for Health and Care Excellence) – Publishes clinical guidelines for lupus diagnosis and management used by NHS specialists.
- Versus Arthritis – UK charity providing information on autoimmune and rheumatic diseases, including lupus, and funding research.
- British Society for Rheumatology (BSR) – Professional body updating UK lupus treatment guidelines and standards of care.
- Which? Healthcare – Independent consumer guide to private healthcare providers and costs in the UK.
This article references current 2026 NHS data and private sector pricing. However, guidance, waiting times, and treatments evolve. Always discuss your individual situation with your GP and rheumatology specialist. Our guide to Raynaud’s disease and scleroderma covers two related autoimmune conditions that sometimes overlap with lupus.
Disclaimer
This article is for information only and does not replace professional medical advice. Lupus is a complex condition requiring specialist diagnosis and management. Never delay seeking medical advice if you suspect lupus or experience any symptoms described above. Always consult your GP or a qualified healthcare professional before making decisions about testing, treatment, or lifestyle changes. If you are already diagnosed with lupus, follow your rheumatologist’s advice and attend all scheduled appointments and monitoring appointments. In an emergency (severe chest pain, shortness of breath, severe headache, or signs of stroke), call 999 immediately.
Share This Guide
If you found this article helpful, please share it with friends, family, or anyone you know who may be navigating lupus symptoms or seeking diagnosis. Early awareness and knowledge can help others get answers faster.
Article published: March 2026 | Last reviewed: March 2026 | Next review due: March 2027